
You can’t forget the price tag when striving for evidence-based care.
Have you ever thought about the cost associated with implementing clinical guidelines?
Evidence-based guidelines have become a cornerstone in clinical management of a wide range of medical conditions. These guidelines are not only becoming more complex, but they are also becoming more expensive.
And although PBS expenditure and MBS contributions have increased by approximately 50% in the ten years to the end of the 2023/24 financial year, the national gross domestic product only grew by about 27% over the same period.
But have you ever wondered how much it would cost to fully implement a set of evidence-based guidelines for all eligible or indicated Australians for a particular condition?
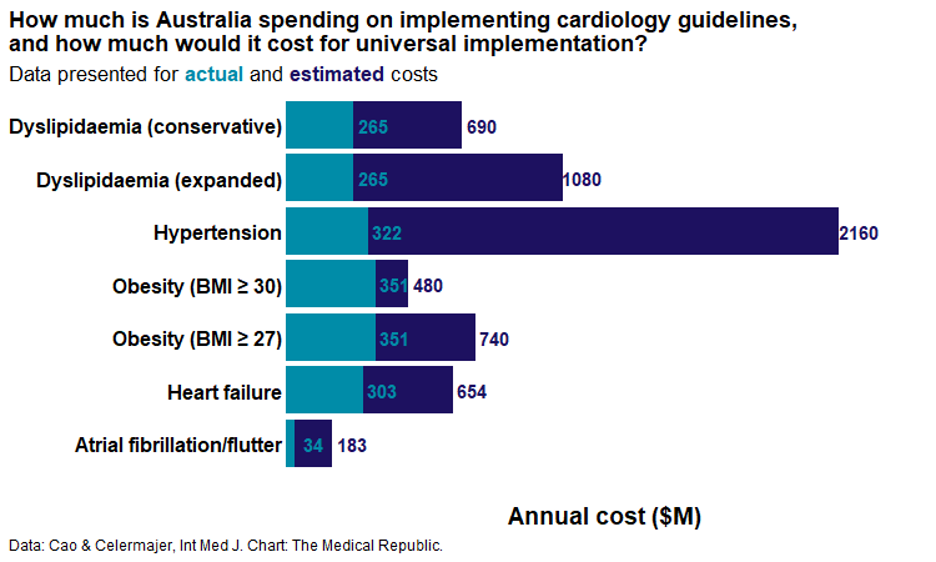
Well, a pair of Australian researchers have. And their findings, published in the Internal Medicine Journal, don’t paint a pretty picture. Their cost estimates for implementing the recommended guidelines for five common cardiovascular conditions sit at 3.4 to 3.9 times the current national expenditure for said conditions.
“By illustrating the scale of the upfront budgetary impact of universal guideline implementation, this work underscores the need for more explicit consideration of economic value alongside clinical benefit,” the authors wrote.
The Sydney-based authors used national population trajectories and Pharmaceutical Benefits Scheme/Medicare Benefits Schedule data to model the expected cost of implementing clinical guidelines for five common cardiovascular conditions in all eligible Australians.
Specifically, they estimated the costs of all eligible individuals receiving:
- Statins and proprotein convertase subtilisin/Kexin type 9 (PCSK9) inhibitors for dyslipidaemia
- Dual antihypertensive medications for hypertension
- GLP1-RAs in for obesity (in people with a BMI ≥ 30)
- SGLT2 inhibitors for type 2 diabetes with consequent heart failure or chronic kidney disease
- Ablation procedures for atrial fibrillation or atrial flutter.
It should come as no surprise that the annual estimated costs for universal guideline implementation were significantly higher than the actual cost spending for the 2024-25 financial year.
The final estimates were 2.6-4.1 times the current PBS spend for dyslipidaemia medications, 6.7 times for hypertension medications, 1.4-2.1 times for obesity-related medications, 2.2 times for T2D with heart failure or chronic kidney disease and 5.4 times the current expenditure on atrial fibrillation or flutter ablation.
“The results of our analyses highlight the complex balance between efficacy, cost and equity in healthcare. We estimated that, across only five common cardiovascular conditions, the projected 10-year cost of full guideline implementation would total ~ $45–50 billion (at 2025 prices),” the authors said.
They identified two key challenges in the way the current system worked. The first was the significant increase in national expenditure that would come with universal implementation of guideline-recommended care. The second, and potentially bigger point, was that many Australians were unable to access or derive benefit from the accepted recommendations that sit within established guidelines.
Related



“Collectively, these findings raise important questions about the long-term equity and sustainability of the Australian healthcare system, even using a limited example of five drugs/procedures from just one body system – the heart,” the authors wrote.
They suggested two potential approaches to overcome these challenges, including cost-effectiveness analyses in the guideline development process and pushing for greater use of cheaper, generic medications.
“An Australian study in 2011 similarly demonstrated a 21% cost saving for patients switching from brand to generic products, but only three in four accepted the change, despite more than 95% of pharmacists recommending it,” they wrote.
“This gap highlights the need for more transparent communication to reassure and educate patients on the equivalence of generics, alongside stronger policy measures to encourage their use.”
While the figures presented by the authors are certainly eye-catching, there are two key limitations to consider when interpreting the results.
“Our 10-year projections assume stable disease prevalence, treatment uptake and medication pricing, which may not reflect real-world trends and would require more detailed disease- and therapy-specific modelling,” they said.
“[In addition,] our analysis assumes full guideline-recommended implementation, whereas in practice, some patients have contraindications or develop adverse effects that preclude therapy, necessitating individual-level data to estimate more accurately.”
