

Autopsies on 12 individuals who died of COVID-19 in Germany has revealed more than half had deep venous thrombosis despite there being no suspicion of this before their deaths.
That’s all for today on the The Medical Republic‘s live COVID-19 blog.
Thanks to our sponsor and supporter for funding this project with an independent grant, Boehringer Ingelheim.
The latest
- Autopsy study of COVID-19 deaths reveals deep venous thrombosis and pulmonary embolism.
- Four funerals and a birthday party …a COVID-19 story from the US that does not have a happy ending.
- Today’s COVID-19 infection figures from around Australia.
- Autopsies on 12 individuals who died of COVID-19 in Germany has revealed more than half had deep venous thrombosis despite there being no suspicion of this before their deaths.
In a prospective cohort study reported in the Annals of Internal Medicine, researchers presented the autopsy findings of 12 consecutive patients with PCR-confirmed COVID-19 who died at a single medical centre.
Two died after unsuccessful CPR, five died in the intensive care unit, and five had advanced directives for best supportive care only and died in the non-intensive care ward.
Laboratory tests for the 10 in-hospital deaths revealed elevated lactate dehydrogenase – a marker of tissue damage – D-dimer, and C-reactive protein. Four of the ten also had mild thrombocytopaenia.
The autopsy found that massive pulmonary embolism was the direct cause of death in four patients, and seven patients in total had deep venous thrombosis, despite that not being suspected before their deaths. Three of these had fresh deep venous thrombosis.
“When hemodynamic deterioration occurs in a patient with COVID-19, pulmonary embolism should always be suspected,” the authors wrote.
The patients’ lungs were all very congested and heavy, with a mean combined lung weight of 1988g compared to standard lung weights of 840g in men and 639g in women.
The authors commented that these heavy, ‘consolidated’ and essentially air-free lungs could explain the difficulties in mechanically ventilating these patients.
Researchers also found high concentrations of SARS-CoV-2 RNA in the lung, and around half the patients also had high viral RNA concentrations in the liver, kidney or heart.
Median age was 73 years, half the patients had coronary heart disease and a quarter had asthma or chronic obstructive pulmonary disease. Three patients were obese and three had type 2 diabetes.
- As Australia contemplates easing some of the restrictions put in place to stop the spread of COVID-19, a study published in the CDC’s Morbidity and Mortality Weekly Report is a timely reminder of the risks of larger social gatherings.
The report documents a cluster of 16 probable and confirmed COVID-19 cases – including three deaths – traced to a single infected person attending a family gathering and funeral in Chicago, followed by a birthday party three days later.
The individual in question had recently travelled interstate and had mild respiratory symptoms but attended a non-COVID-19-related funeral, including a dinner the night before. Four people contracted COVID-19 from those encounters, one of whom later died.
Three days later that same infected person went to a birthday party, which led to another seven people contracting COVID-19, two of whom died. Furthermore, three of those infected birthday party attendees attended a church service six days later, which likely resulted in another infection – in a health care professional.
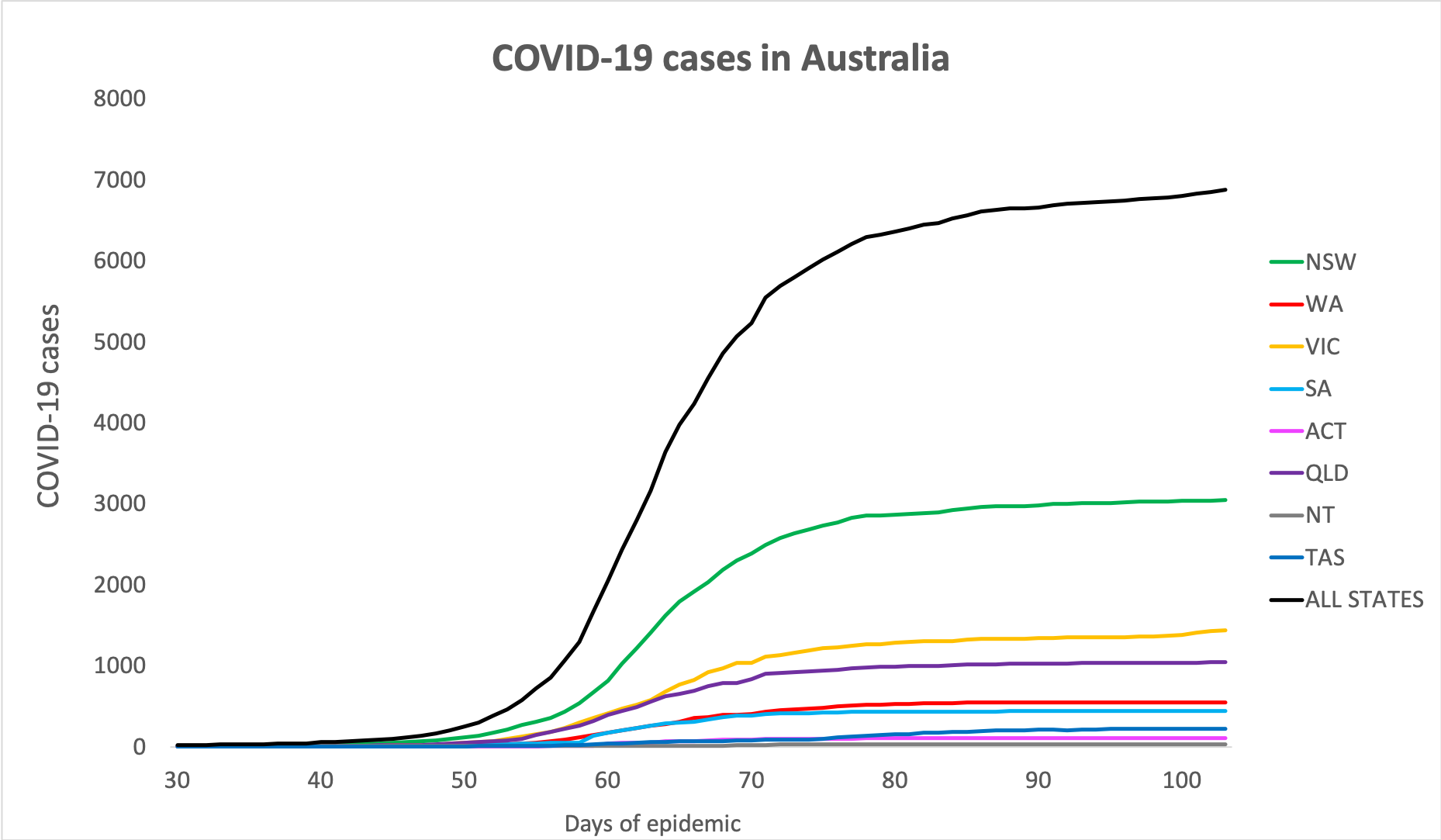
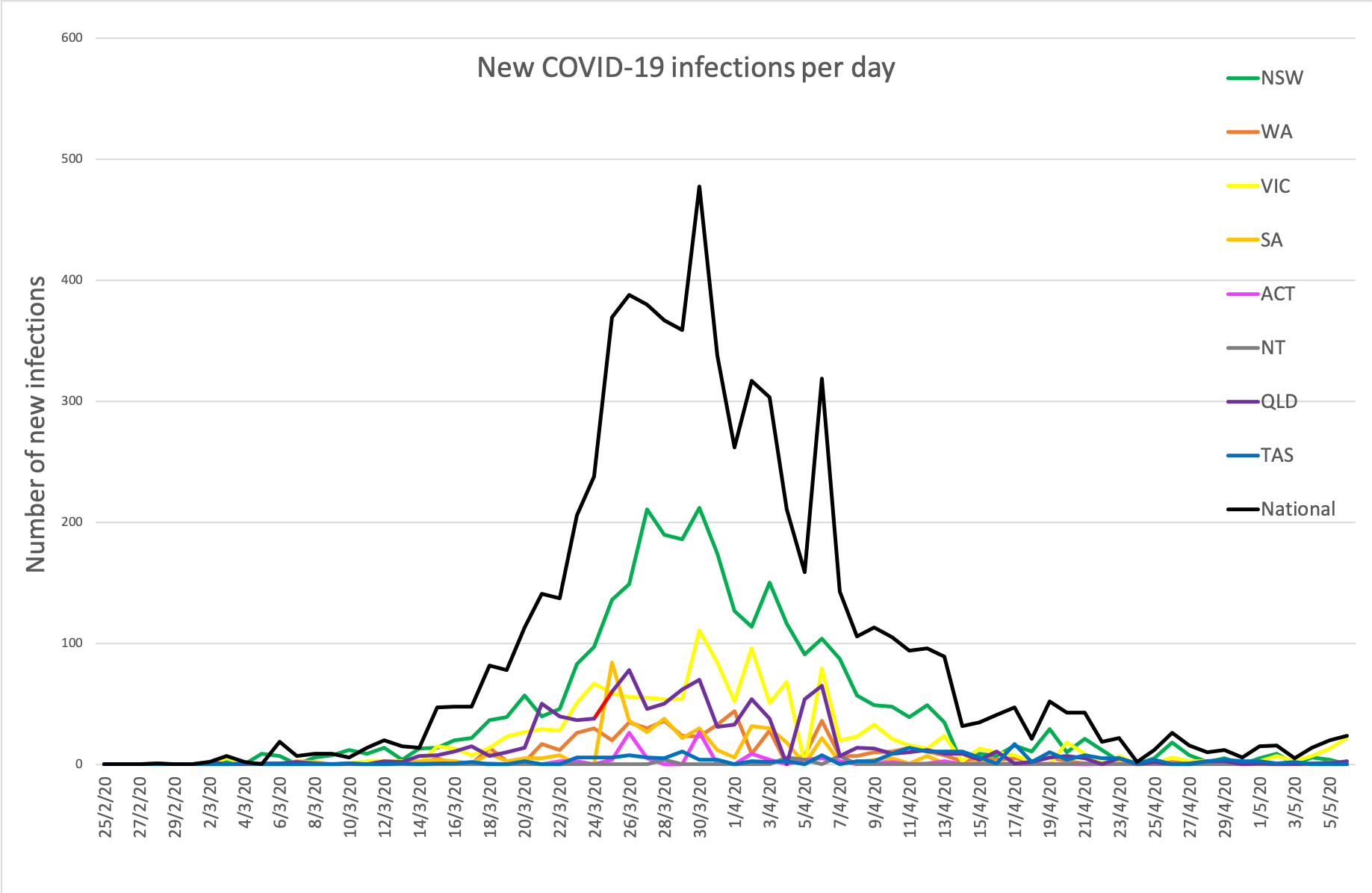
- Here are today’s confirmed COVID-19 infection figures from around Australia to 9pm yesterday. Nearly a week since some states lifted some of their social restrictions and kids went back to school, so we’ll be nervously watching those lines and hoping they don’t start trending upwards.
National – 6875 (up 26) with 97 deaths and 5984 recovered
ACT – 107
NSW – 3042
NT – 29
QLD – 1043
SA – 438
TAS – 225
VIC – 1440
WA – 551
Disclaimer: The content on the Medical Republic COVID-19 blog is independently created by Medical Republic without input from Boehringer Ingelheim Pty Ltd. The views, information, or opinions expressed on the Medical Republic COVID-19 blog are Medical Republic’s own and do not necessarily represent those of Boehringer Ingelheim Pty Ltd. Boehringer Ingelheim Pty Ltd is not responsible for and does not verify the accuracy of any content on the Medical Republic COVID-19 blog.
