The pressure is on again to return to bulk billing so we can compete with non-doctors. We have to resist.
As part of educating myself on finance and small business ownership better, I follow several finance “bros”, among them this guy, who recently tweeted this ad from the 90s:
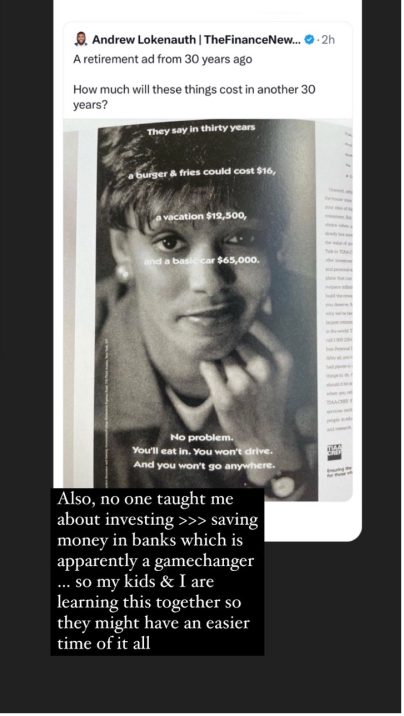
Inflation is a given, yet most of us, self-employed or not, remain blissfully aware of its impact on us on a day-to-day basis, until it suddenly feels impossible to manage.
This is why so many of us, used to bulk billing, sleepwalked into the crisis that a decade of frozen Medicare rebates led us to in the last year or two. That’s why the public anger continues to boil and simmer at those of us who suddenly dare to charge gap fees.
The latest of this, of course, is the ongoing threat of task substitution by non-GPs – MBBS doctors post-internship masquerading as fellowed doctors selling drugs online on demand; nurses and nurse practitioners running a “general practice” that is entirely bulk billed as they are not bound to the 12-month face-to-face rule GPs are; and of course, the continuing encroachment by the Pharmacy Guild on to our work, under the guise of convenience and access for the “simple things”.
Having drifted for so long, course correction to make up for 11 years of frozen rebates looks like “greed”.
What lessons can we learn?
A friend who’s moved to 100% private billing – and is still booked out two to three weeks in advance – pointed out recently that, in the face of all this task substitution, it feels like they want us to simply capitulate and return to bulk billing, or else we won’t be able to compete.
The only way to survive and thrive, as I see it, is to stick to our new path.
What is in the best interest of ourselves as service providers and our patients?
It is to stay viable.
It is to survive and then to thrive.
It is to raise fees annually or more often as needed in line with inflation at minimum, to allow us to continue to operate our practices; to pay our staff living wages; to continue to invest in ongoing professional development and more.
It is to have enough left of our take home pay that we are not reliant on a salaried or wealthy spouse to subsidise our life because we aren’t making enough to pay our own bills.
All of this is hard.
Related



In the face of the impending pressures from government and other non-GPs who offer the promise of “fast, cheap AND as good”, it is easy to consider capitulating.
Scarcity mindset sets in. We find ourselves worrying we’ll be out of work soon enough if we don’t give in.
Except …
I was there in 2013 when the vast majority of GPs were still bulk billing, including my supervisors at the practice I was in as a final-term registrar awaiting fellowship.
I was also working in one of the lowest SES areas in Sydney, where everyone told me “They won’t pay. You’ll lose money and cost us money.”
I charged gaps anyway, because I’ve never been able to do “churn and burn” medicine and it felt soul destroying to me to have a patient come in, order a script and walk out.
It took time, but nothing catastrophic happened.
When I moved to my next practice a year later, some of the patients followed me there.
Then to my next practice again, which was 100% private billing.
The other day I had a patient who used to see me pre-covid and who messages me every year or so to ask if I’m back in the CBD as she would “love to see you again if you are”. Alas, I am not.
Patients who can afford to pay for good care usually care more about the value of the service and less about the actual dollar value. They’re also usually the people who want a doctor, not a substitute. Usually, they also understand that all businesses have running costs and that prices need to go up regularly to keep up with these.
By charging the majority reasonable prices for my services, I’ve always – until this particularly tight year – been able to have a handful of people whom I either discount or bulk bill, or to do bulk bill-only work at a low-SES clinic.
So if you feel guilty about charging gap fees … if you feel bad, and greedy … if you fear that you have “no choice” but to give in, and race to the bottom to compete with the non-GPs …
Stop.
The need for great GPs is only going to grow. A good GP who provides excellent value will become worth their weight in gold because the rest will be competing for bulk-billed, convenient but fragmented care. They are not your ideal patients. Let them go.
Focus on your skillset. Focus on the service you offer, erect effective boundaries and provide excellent care.
If you do this, you risk becoming like the non-GP specialists so many of us moan about – “they can charge exorbitant fees because there are so few of them, they have a market share”.
This is your opportunity to do likewise if you wish. In exchange, you can give your skills for less or for free to a few if you wish to.
Above all, learn some basic financial literacy and at minimum, raise your prices every year in line with inflation at minimum so you are not running at a loss.
Dr Imaan Joshi is a Sydney GP; she tweets @imaanjoshi.
