
CASE STUDY: Knowledge of ankle arthroplasty components and review of prior x-rays helped deduce the cause.
A 61-year-old female patient presented with an 18-month history of painless clicking in her ankle.
This ankle had undergone total ankle arthroplasty approximately nine years ago due to severe osteoarthrosis secondary to systemic lupus erythematosus.
On examination, the patient was ambulant and functioning well, but noticed a clicking sensation on walking. Due to travel restrictions (this patient was from interstate), she was unable to attend her ankle surgeon’s consultation for 18 months and finally presented to our clinic for radiographs and CT to further evaluate the cause.
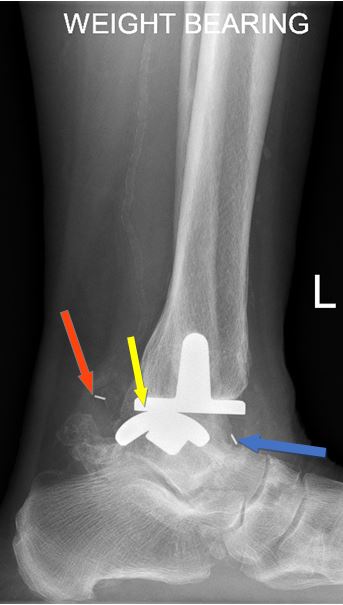
The radiographs reveal a pronounced loss of joint space, with relative posterior translation of the talar component compared to the tibial component. There is the additional presence of metallic markers in the anterior and posterior tibiotalar joint along with small osseous fragments.
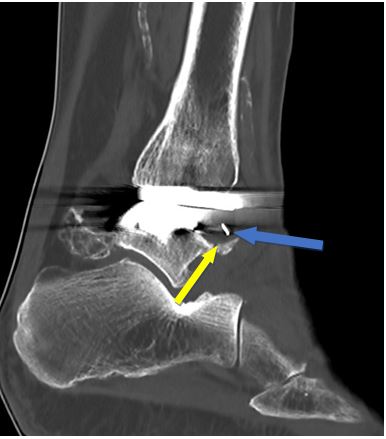
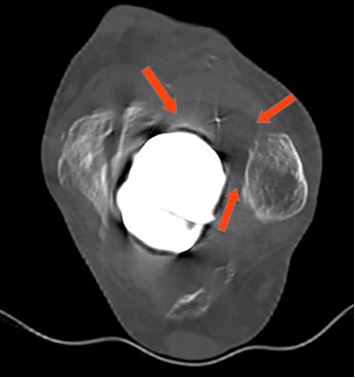
On CT, these markers are better visualised and belong to fractured elements of the polyethylene liner, which can be seen as radiolucent circumscribed material in the anterior and posterior ankle joint. In addition, there is indolent bone erosion over the anterior margin of the talar component presumably due to chronic impingement from the polyethylene fragment lodged in the anterior ankle joint and the posterior talar subluxation.
These features are even more striking when prior x-rays dating back to the postoperative period are reviewed, making the loss of joint space, bony malalignment and the displaced polyethylene markers are more apparent.
This case is a rare presentation of fracture of the polyethylene mobile bearing and although one may not have encountered such a presentation previously, the pathology can be deduced when there is an understanding of the components of ankle arthroplasty along with review of prior radiographs to see the relative change.
Figure A – lateral ankle radiograph demonstrating the presence of metallic markers in the anterior (blue arrow) and posterior ankle joint (red arrow). Note the reduced joint space and the posterior positioning of the talar component relative to the tibial component (yellow arrow).
.
Figure B – Frontal ankle radiograph from 2022 showing loss of joint space. Note that the metallic markers are not visible as they are superimposed on the more dense arthroplasty components.

.
Figure C,D; E,F – Sagittal (C,D) and Axial (E,F) CT images showing the metallic markers (blue arrows) and lucent outline of polyethylene (red arrows). On the sagittal view there is bony remodelling and erosion at the anterior talar component’s margin (yellow arrow).


.
Figure G,H: Review of x-rays performed in 2013 shows the polyethylene markers are in the midline (blue arrow) between the talar and tibial components. Note the normal alignment and joint space.


Dr Sebastian Fung is a musculoskeletal radiologist who undertook an MRI imaging fellowship in Hospital for Special Surgery in New York. He now works in Sydney at St Vincent’s Private Hospital and Mater Hospital.
