
What would general practice look like if GPs weren’t expected to hold the whole system together alone?
If you’re a GP reading this, the next few lines may feel uncomfortably familiar.
Monday morning. Dr Sarah’s waiting room. 8:07am. Four patients already waiting.
The first patient is 68. Diabetes. Early heart failure. His wife died two years ago. He lives alone. He’s here because his blood sugar is up again.
Sarah spends 15 minutes adjusting his medication and books a follow-up in three weeks.
What she doesn’t have time to ask: Has he eaten today? Is anyone checking in on him? Is he taking the medication, or are the tablets still sitting unopened in a drawer because he can’t read the labels anymore?
Sarah already knows the answer. She’s been his GP for nine years. But there are three people in the waiting room.
The system isn’t built for that conversation.
The second patient is 44. Two kids. Night shifts. Exhausted.
She’s had four appointments in six weeks. Each time a different issue: a shoulder strain, poor sleep, a rash that cleared up. Sarah notices the pattern.
What this woman needs isn’t another prescription. She needs support. Maybe a mental health practitioner. Maybe a social worker. Maybe someone who can help stabilise the chaos around her life.
Sarah refers her to a mental health service. There is an eight-week wait.
By lunchtime Sarah has seen 18 patients.
She’s running 40 minutes late. She hasn’t had a coffee. And she’s writing referrals to services she isn’t confident will see her patients any time soon.
This isn’t burnout. It’s architecture.
Burnout isn’t what happens when doctors care too much. It’s what happens when systems ask them to hold everything together alone.
Now imagine Tuesday. Same GP. Same patients. Different system.
Dr Sarah now works alongside a Neighbourhood Health Hub, a multidisciplinary team serving the local community.
In many integrated health systems internationally, neighbourhood care teams serve 30,000–50,000 residents, bringing together general practice, community health, mental health and social care around the same population.
When the 68-year-old with diabetes comes in, Sarah doesn’t just adjust medication. There’s a social prescribing link worker two doors down.
Related

She does a five-minute warm handover. The link worker spends an hour with him, not as an afterthought, but as a designed part of his care.
By the end of the week:
- a community pharmacy is organising blister-packed medication;
- he’s connected to a men’s group nearby;
- a community nurse is included in his care plan.
His next admission to hospital isn’t inevitable. It’s preventable.
The 44-year-old doesn’t wait eight weeks. The hub has a mental health practitioner embedded in the GP team. Same building. Same care network. She’s seen within days.
Sarah still has a full waiting room. But she isn’t carrying the system alone anymore. And that changes everything.
Over the past several decades working in healthcare, I’ve heard the same response from clinicians across Australia:
“It sounds good in theory.”
So, let’s be specific about what actually changes.
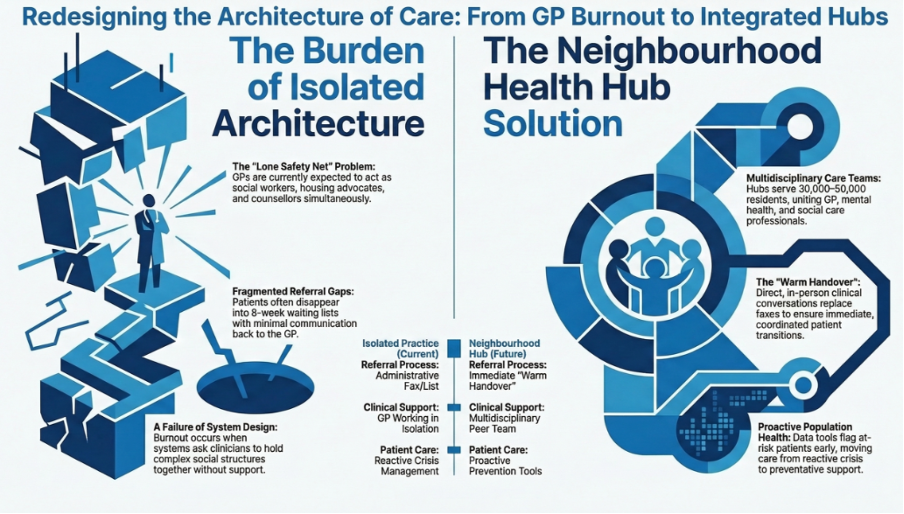
You get a team, not a referral list
In today’s system, referrals often mean losing patients. They disappear into waiting lists, different organisations, or services that rarely communicate back.
In a neighbourhood health hub, allied health professionals are part of the same working team – physiotherapists, mental health clinicians, social workers, pharmacists, community nurses.
The handover is a conversation, not a fax.
Every GP knows the patients who occupy the most cognitive space — not because of one diagnosis, but because of everything else happening in their lives:
- chronic disease;
- mental health;
- housing stress;
- social isolation.
In a hub model, those patients are supported by a care coordinator, someone whose job is to hold the threads between services.
You still make the clinical decisions, but you’re no longer trying to be the social worker, housing advocate and family counsellor all at once.
Prevention becomes possible
Population health tools allow teams to identify people at risk before they deteriorate. Instead of waiting for the 68-year-old to arrive in crisis, the system flags him earlier. Someone reaches out.
Support happens earlier.
The GP appointment becomes part of a continuum of care rather than the final safety net.
You belong to something bigger than your practice
Isolation is a real problem for GPs – long hours, complex decisions, limited opportunities to debrief.
Neighbourhood health hubs change that. You’re connected to a multidisciplinary team. You share complex cases. You learn from colleagues you might otherwise never work alongside – the physiotherapist who spots the mental health signal; the social worker who understands the family dynamics; the community nurse who has seen the home environment.
That collective intelligence makes you a better clinician. And it makes the work sustainable.
The honest bit
None of this is easy to build. It requires:
- governance that spans organisations;
- funding models that reward coordination instead of activity;
- digital infrastructure that allows clinicians to share information across services;
- And it requires a shift in how we think about general practice.
Not as the beginning of a referral chain, but as the centre of a care network.
Because the Monday morning I described at the beginning isn’t a failure of Dr Sarah. It’s not even a failure of intention. It’s a failure of architecture.
And architecture can be redesigned.
The real question is this:
What would general practice look like if GPs weren’t expected to hold the whole system together alone?
Eugene McGarrell is general manager of commissioning and planning with the Sydney North Health Network, and former CEO of Health Australia.
This article was originally published on Mr McGarrell’s LinkedIn feed. Read the original article here.
