

The modelling that underpins Australia's COVID-19 pandemic response strategy has been released by the Prime Minister and the Peter Doherty Institute for Infection and Immunity at Melbourne University.
That’s all for today from The Medical Republic‘s live COVID-19 blog.
Thanks to our sponsor and supporter for funding this project with an independent grant, Boehringer Ingelheim.
Any questions, comments or confirmations? Email bianca@biancanogrady.com.
The latest
- The modelling underpinning Australia’s COVID-19 response is released.
- The Prime Minister has announced a mandatory code for commercial tenancy, which could help GPs.
- Could fever clinics help take some of the COVID-19 burden and risk away from hospitals?
- Outpatient fever clinics can take a significant workload off hospital emergency departments and potentially reduce spread of COVID-19 in hospital environments, new data suggests.
A retrospective non-peer-reviewed study published on the preprint server MedRxiv looked at the effect of establishing a COVID-10 fever clinic at the Peking Union Medical College Hospital in China.
Overall, more than 6000 patients were screened at the clinic over 40 days. After the outbreak began, fewer patients were transferred from the fever clinic to the hospital emergency department, and patients spent significantly more time in the fever clinic compared to before the outbreak
“The work-load of the FC [fever clinic] increased after the COVID-19 outbreak and effectively prevented COVID-19 from spreading in the hospital as well as offload ED resources,” the authors wrote.
- Penny Durham reports: Two studies have been released after weeks of clamour to “show us the modelling”.
These are from the Peter Doherty Institute for Infection and Immunity at Melbourne University, which has worked with the government previously on pandemic influenza modelling.
Both the PM and the CMO today stressed, however, that these studies were highly theoretical, were not based on Australian data, did not take into account Australian mitigation measures, and could not be used to make predictions about our COVID-19 course.
With all those caveats out of the way, Professor Murphy said the institute had modelled what would happen in the “highly artificial and very unlikely” scenario the whole country was infected.
Without mitigation measures, unsurprisingly, that would result in 35,000 ICU presentations a day – a “horrendous scenario” beyond any health system’s capacity.
Quarantine and isolation measures would blunt that peak somewhat, but social isolation measures were what achieved real flattening of the curve.
Professor Murphy said Australian measures to date already exceeded what was modelled in the more extreme distancing scenario and our actual data reflected that projected slowing.
But he said it was essential that we maintain all those measures to keep the outbreak under control.
- From TMR reporter Penny Durham: The Prime Minister has announced a mandatory code governing tenancy agreements during the pandemic, in a move that may bring a little more certainty to general practice.
TMR has heard from multiple sources that pathology tenants are reneging on their rental agreements, threatening to put another hole in general practice income.
Scott Morrison said this afternoon that the “legislated and regulated” code would prohibit a commercial landlord from terminating a lease or drawing on a tenant’s security, and would require a tenant to honour their lease.
This applies to businesses in distress (either landlord or tenant) with a turnover of $50 million or less.
Tenants are, however, entitled to request a rent reduction proportionate to their business they have lost during the crisis.
This would come in a combination of waivers and deferrals of rent. Waivers must account for at least 50% of the reduction of the rental, and deferrals must be covered over the balance of the lease term, giving tenants a minimum of 12 months to pay.
This will be overseen through binding mediation processes run by the states and territories.
News of the downturn in regular GP visits has permeated up to the Department of Health, prompting Chief Medical Officer Brendan Murphy to issue a plea to the public to keep up with their medical appointments.
At today’s press conference he said he was very concerned to hear that people with conditions other than COVID-19 were no longer getting their checkups, for fear of leaving their homes and visiting doctors’ rooms.
“Please don’t neglect general health conditions at the moment,” he said.
He urged the public not to put off seeing their GP, but of course to ring up first and potentially seek a telehealth appointment before visiting in person.
12.50pm, 7 April
- Need more information on the suspension of GP practice accreditation assessment cycles, which was announced a couple of weeks ago? The Australian Commission on Safety and Quality in Healthcare – which runs the accreditation process using the RACGP’s standards – has published an FAQ about the situation, which explains what the suspension means for your practice, how it will operate and the impact on eligibility the Practice Incentives Program and Workforce Incentive Program.
For example, it says onsite assessments will recommence once the pandemic has entered the recovery phase. The number of days since the suspension will be calculated and added to your practice’s current accreditation certificate expiry date. The practice will then need to schedule an assessment with its accrediting agency to be completed before the revised expiry date.
- Queensland is expanding the COVID-19 testing criteria in Brisbane, Cairns and the Gold Coast. Anyone presenting with acute respiratory symptoms of unknown origin can be tested, even if they haven’t travelled recently, haven’t had contact with a confirmed case or aren’t working in healthcare.
The announcement comes as those cities record cases with an unknown source of infection, and the government moves to reduce the likelihood of sustained community transmission.
Testing criteria for coronavirus (COVID-19) will be increased in Cairns, Gold Coast and Brisbane as a precaution following the detection of cases with unknown sources of infection. The increased testing has been ordered to head off the risk of sustained community transmission. pic.twitter.com/e6r2r38Vbt
— Queensland Health (@qldhealthnews) April 7, 2020
11.05am, April 7
- Want to learn from frontline experiences in managing severe COVID-19 pneumonia? The Asia Pacific Association of Critical Care Medicine is hosting a live Zoom webinar this Saturday at 4pm AEST, featuring speakers from China, New Zealand and Singapore. To join in, go to split.to/managecovid19.
Don’t miss the live webinar on Saturday 11th April on Management of severe COVID-19 pneumonia: Experiences from the frontline. Check out the flyer for more information. pic.twitter.com/0IrBovOp3v
— ANZICS (@anzics) April 6, 2020
- A second study points to a possible role for plasma transfusions from patients who have recovered from COVID-19 to those who are still suffering severe infection.
A paper published today in PNAS presents outcomes from a prospective pilot study in 10 adults hospitalised with severe COVID-19. They were given one 200 mL dose of plasma collected from patients who had had COVID-19 but had been discharged from hospital with normalised temperature, resolution of respiratory symptoms, and two negative sputum tests for SARS-CoV-2.
After the transfusion, levels of neutralising antibodies against SARS-CoV-2 increased rapidly in half the patients. Within one to three days, all showed improvements in symptoms such as cough, fever, shortness of breath and chest pain. They also showed reduced markers of inflammation, and seven patients had undetectable viral loads within two to six days after the transfusion.
“These results are in support of a neutralising effect of CP [convalescent plasma] on serum SARS-CoV-2,” the authors wrote.
Most importantly, there were no serious adverse effects or safety concerns associated with the transfusion.
- Around one-quarter of patients admitted to intensive care with COVID-19 in Lombardi, Italy, have died, according to a case series. In a paper published in JAMA this morning, researchers presented analysis of 1591 critically ill patients; 99% of whom needed respiratory support, mostly intubation but 11% had non-invasive ventilation.
The median age was 63, four-fifths of patients were male, and around two-thirds had at least one comorbidity.
The most common was hypertension, which was present in nearly half of patients. One in five patients had cardiovascular disease, and 18% had hypercholesterolaemia.
Overall mortality was 26%, but was lower (15%) in those aged under 63 years and higher (36%) in those aged over 63. The study also found that patients who died were significantly more likely to have hypertension than those who were discharged from the ICU.
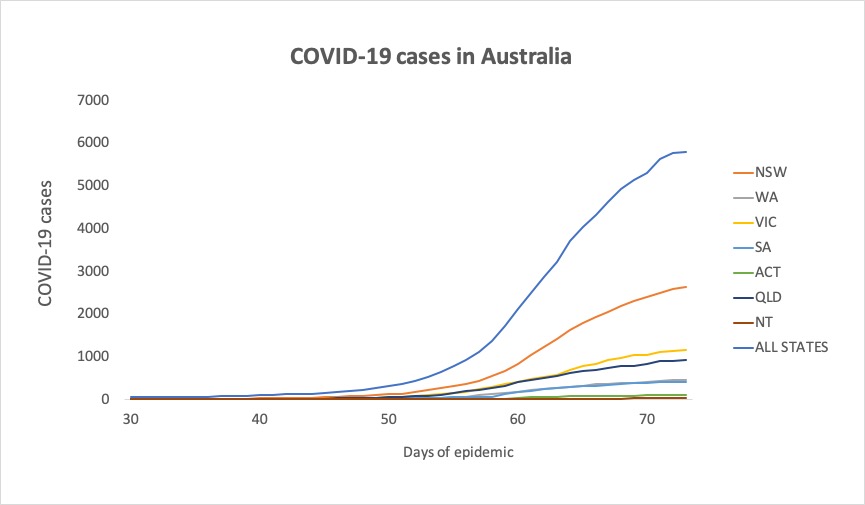
- Here are the infection stats since 3pm yesterday:
National – 5,795 (up 108) and 39 deaths
ACT – 96
NSW – 2637
NT – 27
QLD – 921
SA – 411
TAS – 85
VIC – 1158
WA – 460
And in chart form, so we see what is hopefully a flattening of the curve:
- Media reports that the Federal Government is finally going to release its modelling of the COVID-19 pandemic today. According to the ABC this morning, there are mixed feelings about the release, with some experts concerned the data will be misinterpreted but others arguing that the government’s actions on COVID-19 – such as the lockdown and closure of parliament – need to be understood and judged against the evidence for their effectiveness.
- Science was pretty quiet on the COVID-19 front yesterday, but politics and regulatory stuff was running hot. The big story was that GPs can now bill privately for telehealth items, except for concession card holders, children, and those at high risk of COVID-19. A report suggested the private health industry was likely to do very well indeed from this pandemic, as reduced demand for services could see it get a multi-billion-dollar windfall. Australian clinicians now have access to ‘living’ guidelines on COVID-19, put together by a large coalition of Australian health professional groups. And a tiger in the Bronx Zoo in New York tested positive for SARS-CoV-2. Poor kitty.
Disclaimer: The content on the Medical Republic COVID-19 blog is independently created by Medical Republic without input from Boehringer Ingelheim Pty Ltd. The views, information, or opinions expressed on the Medical Republic COVID-19 blog are Medical Republic’s own and do not necessarily represent those of Boehringer Ingelheim Pty Ltd. Boehringer Ingelheim Pty Ltd is not responsible for and does not verify the accuracy of any content on the Medical Republic COVID-19 blog.
