
In the immortal words of Ferris Bueller, ‘it’s over, go home’. Why did the college ignore advice to better protect its members?
In this week’s update to the definition of general practice for accreditation purposes the RACGP chose to go out with the good news PR angle that the new definition would now capture “good” telehealth and quite specifically exclude “bad” telehealth.
Good telehealth providers, according to the college, are models that retain the longitudinal and holistic qualities that underpin good general practice, and include previously excluded but important areas such as those entities delivering services to aged care facilities. Bad telehealth providers are generally those platform-based single-disease indication services. You can read more about the college’s logic here.
All of this is pretty sensible and good stuff. It will mean that certain important adjunct general practice services will now be able to access the lucrative WIP and PIP programs through which single practices can earn themselves up to $180,000 more per year.
But the good news on telehealth wasn’t the real story of this update.
The real story was that despite a lot of warnings and advice about adjusting the wording of the definition and some processes in order to account for what is probably the largest and most important administrative and financial crisis facing general practice – payroll tax – the college chose, quite knowingly it appears, to ignore the problem altogether.
The problem, in a nutshell, is that the way the definition of general practice has been crafted in the accreditation standards is rich fodder for any state revenue office to use in any audits it does on any accredited practice, or indeed in any court case that might ensue.
The way the fifth and previous editions are written in essence says to any SRO in the country that if you want a way to ping a practice for centralised command-and-control type administration and management that points to them being a “medical practice” with “employees” rather than a mere “administrative entity” running a shopping centre-type service model for “tenanted doctors”, then read their accreditation contract. It’s replete with wording and processes that proudly announce that this practice has signed up to exactly the sort of structures and processes you are looking for.
You can read the 5th edition of the Standards for General Practice here.
Check out specifically core standard 3, which is a “how to” guide to running an accredited practice if you want to fall foul of an SRO payroll tax audit. Some choice wording in point summaries appears below.
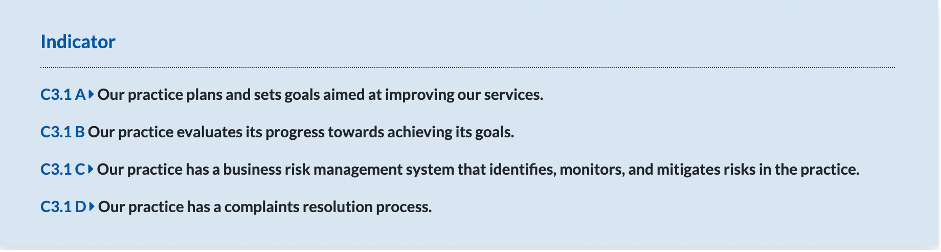
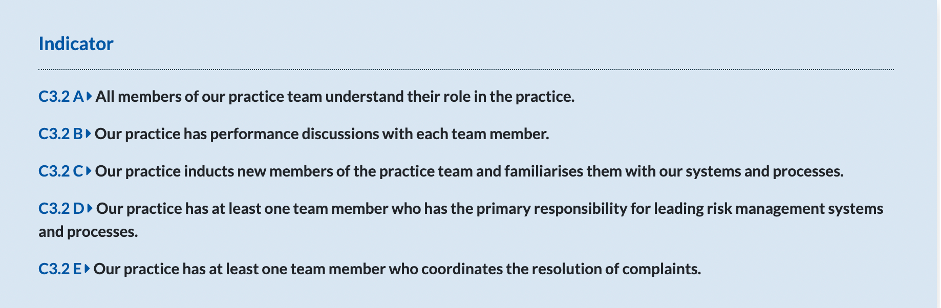
Why would the college simply ignore advice warning that if they didn’t tweak all this wording and some processes in these standards in the right way, they would be creating a potentially huge payroll tax rod for every accredited practice’s back?
It most likely starts with the perspective of nearly every GP and GP practice owner that the reason they exist is to deliver the very best of care for their patients and that everything outlined in the standards, particularly around being patient-centric and having to be team-based to optimise care, makes perfect sense.
It does of course, so it’s understandable and completely natural for GPs to be revolted by the idea of rewording all of this in a manner that might dilute their commitment to good quality longitudinal and team-based patient care.
But by not rewording it the RACGP has exposed every accredited practice to significantly more risk of failing an SRO payroll tax audit.
During the feedback and review process for developing the 5th edition of the Standards the college got direct feedback from some accountants and lawyers that they didn’t need to significantly overhaul anything in order to reduce practice exposure to this problem. Although not obviously tested (and now it can’t be because the advice was ignored), the advice was that the college simply needed to reword various parts of the standards in order to indicate that the centralised services and team-based care in place within the practice was all a part of the operational agreements with the “administrative entity”.
We know the RACGP doesn’t want to expose any of its members to any more payroll tax risk than they currently have so why did they choose to not make what we are told are reasonably simple adjustments?
If you read what RACGP vice president Dr Michael Clements told The Medical Republic about why the college chose to ignore the problem you will likely struggle, like me, to understand what is going on.
Dr Clements said that there were behind-the-scenes challenges in designing standards and policies while trying to take into account the state-by-state interpretations of tax rules.
“We have to be careful not to change general practice or change our standards and the way good general practice operates just because we’ve got one or two recalcitrant states that are still deciding that they want to tax patients for accessing healthcare,” he said.
“We actually think the solution for payroll tax is not that the general practices stop doing what they do and working for the betterment of the patient.
“The solution to payroll tax is the state governments keep their hands out of the patient-doctor interaction.”
One or two recalcitrant states? No – every state and territory, maybe with the exception of WA.
And who is “we”?
Because if it is the RACGP then apparently the reason the college has ignored this very significant problem for their members in their new version of the standards is because state governments have to grow up and just “keep their hands out of the patient-doctor interaction”.
In other words, the college is still clinging to the dream that they will get every state government to change tax law for them. Not changing the wording in the standards then looks like some sort of wilful disobedience.
Related


The horse that says that somehow state governments will listen to the argument that “we are doctors and this is the best way to treat our patients so you need to change tax law that has existed forever and applies to every other professional group, because a lot of us have unfortunately slept-walked into practice structures that don’t meet that law”, bolted some time ago.
Surely what is now happening in South Australia should have woken up anyone out there still clinging onto this fever dream.
After a meeting with the SA treasurer this week in a last-ditch effort to somehow reignite the dream, an AMA spokesperson admitted that “unfortunately there is no indication that the treasurer and his team in RevenueSA will change their decision to implement the tax”.
Even that wording has the whiff of ongoing denial about it.
The tax isn’t being implemented. It exists and has for over a decade in SA in its current form. All RevenueSA has done is quite recently realise that a lot of GP practices have business structures that are non-compliant with payroll tax. It then trickily got a whole lot of them to lift the bonnet and show them that indeed they are non-compliant, enforcing long existing state tax law.
Every state has in various ways rebutted every argument and effort by the AMA and the college to get this dream up, not just SA or a couple of “recalcitrant” ones.
In the immortal words of Ferris Bueller, “everyone, it’s over, go home…”
You can make your own judgement on Dr Clements’ reasoning for ignoring the problem in the new edition of the standards and whether his view is the view of the college as well, as it appears to be.
I’m sure nearly everyone agrees with the sentiment of what he has said: of course general practice needs to work in a team-based manner to optimise care.
But that does not mean the college shouldn’t be a lot more pragmatic here and do what they were advised to do by the accountants and lawyers and fiddle with the wording just a little in order to create a lot more protection for their members.
Calling an administrative entity a practice for the sake of accreditation is exactly what the SROs are looking for.
If it’s pride that’s at stake then swallow it for the greater good. Play the game much better on behalf of your members.
