CASE STUDY: Weightlifting-related microtrauma causes bone degeneration in a 25-year-old male patient.
This 25-year-old male patient presented with gradual onset dull aching shoulder pain following an increase to his exercise regimen, including bench pressing and weightlifting.
There was no antecedent defined traumatic event. Pain was aggravated with repetitive overhead movements or loading the acromioclavicular joint, improving when these activities were avoided and then worsening on resumption of these activities.
On physical examination there was pain with palpation over the area of the acromioclavicular joint. Strength was preserved and range of motion was only limited by pain.
On MRI, there is intense marrow oedema at the lateral end of the clavicle abutting the acromioclavicular joint, but no oedema on the acromial side. This is associated with linear low signal in the subchondral bone likely denoting an insufficiency fracture. The intra-articular disc, usually low signal, is torn and poorly visualised and there is a small effusion as well as capsular thickening.
This was diagnosed as distal clavicular osteolysis with associated insufficiency fracture This is an injury which affects typically athletes who perform repetitive overhead movements, such as weightlifters, as they sustain repetitive excess load to the acromioclavicular joint, typically through horizontal adduction, adduction, internal rotation and forward/lateral flexion of the shoulder.
The resultant microtrauma to the subchondral bone of the distal clavicle causes subchondral cystic changes, disruption of the articular cartilage, and metaplastic bone formation with increased osteoclastic activity and “osteolysis”.
Conservative management is usually effective and involves activity modification or abstinence, nonsteroidal anti-inflammatory medications and physiotherapy. Surgical resection of the lateral clavicle for patients not responding to nonoperative management or athletes unable to modify specific athletic tasks is also often effective.
Dr Sebastian Fung is a musculoskeletal radiologist who undertook an MRI imaging fellowship in Hospital for Special Surgery in New York. He works in Sydney at St Vincent’s Private Hospital and Mater Hospital.
Image 1a: Coronal fat saturated image of the acromioclavicular joint showing marrow oedema only on the clavicle side (red arrow). Note the linear low signal in the lateral clavicle indicating a fracture (blue arrow).
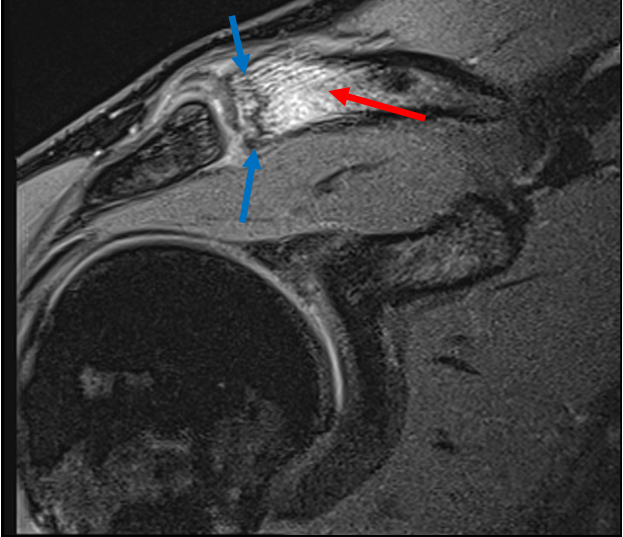
Image 1b: Coronal T2 fat saturated image of a normal AC joint for comparison.
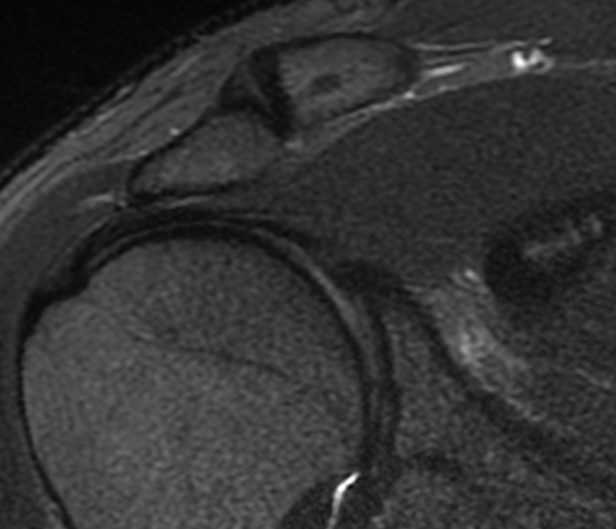
Image 2a: Coronal PD sequence showing the linear low signal fracture line lateral distal clavicle (blue arrow).
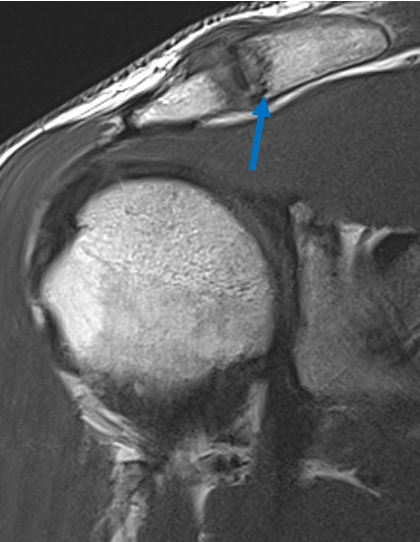
Image 2b: Coronal PD image of a normal AC joint for comparison.
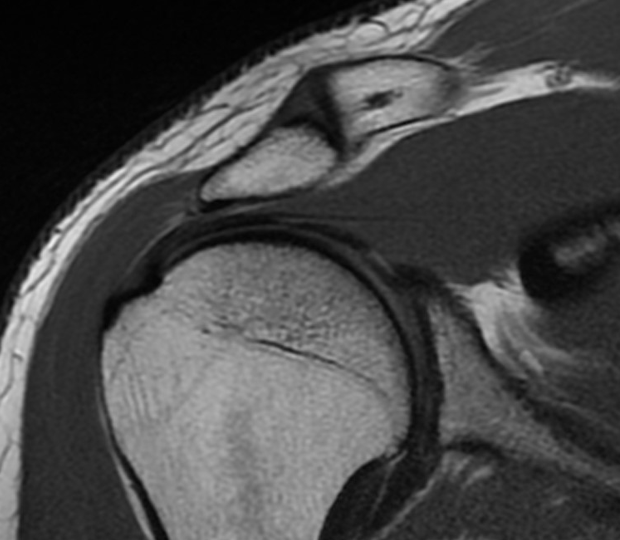
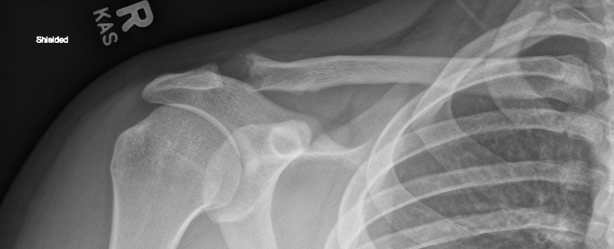
Image 3: X-ray of distal clavicle osteolysis