

Self-collection of nose and throat swabs could be an option to reduce healthcare workers’ exposure to patients possibly infected with COVID-19
That’s it for today on The Medical Republic‘s live COVID-19 blog.
Thanks to our sponsor and supporter for funding this project with an independent grant, Boehringer Ingelheim.
The latest
- Could patient self-collection be used to test for SARS-CoV-2? Australian prepress study suggests yes.
- Victoria expands COVID-19 testing criteria to any unexplained acute respiratory infections.
- Majority of pregnant women with COVID-19 infection may be asymptomatic, case series suggests.
- Self-collection of nose and throat swabs could be an option to reduce healthcare workers’ exposure to patients possibly infected with COVID-19.
An Australian study, published on the prepress server MedRxiv, asked 236 patients attending two dedicated COVID-19 testing clinics to do self-collection with a nasal and throat swab before having a second swab done by a healthcare worker. The PCR testing of both swabs showed a high level of agreement between the self-collected and healthcare worker-collected samples, both for SARS-CoV-2 and other respiratory viruses.
“Self-collection also provides patients with easier access to testing, reduces the exposure of the community and health workers to those undergoing testing and reduces the requirement for PPE,” the authors wrote. - Telehealth item numbers linked to the Veterans’ Access Payment are now available, and the VAP fee has doubled for face-to-face and telehealth services, according to the RACGP. There had been some issues with getting the Veterans’ Access Payment for telehealth items, so the Department of Veterans’ Affairs has set up two new VAP item numbers: MT88 (instead of 10991) and MT89 (instead of 10990).
- Victoria has expanded its COVID-19 testing criteria to include anyone with fever or symptoms of acute respiratory infection that does not have an alternative diagnosis.
The state’s Chief Health Officer Brett Sutton issued the new advice this morning in an effort to combat community spread of the infection. The specific wording is to test patients with “fever or chills in the absence of an alternative diagnosis that explains the clinical presentation or acute respiratory infection that is characterised by cough, sore throat or shortness of breath.”
Testing is also recommended for people who have new onset of clinical symptoms such as headache, myalgia, runny nose, loss of sense of smell, nausea, vomiting or diarrhoea, and who are either close contacts of a confirmed COVID-19 case or who have returned from overseas in the past two weeks.
Patients who are tested should isolate themselves at home until their test results are available.
- More than one in ten pregnant women screened for COVID-19 when admitted for delivery in New York was found to be infected despite having no symptoms, according to a letter in the New England Journal of Medicine.
Doctors screened 215 pregnant women for COVID-19 on admission to two New York hospitals between March 22 and April 4. Four women had COVID-19 symptoms including fever, and all four tested positive for SARS-CoV-2.
However 29 women (13.7%) of the 211 asymptomatic women also tested positive for SARS-CoV-2, which meant nearly 90% of those with the infection had no symptoms. One patient who initially tested negative had a positive swab test three days later.
“Although this prevalence has limited generalisability to geographic regions with lower rates of infection, it underscores the risk of COVID-19 among asymptomatic obstetrical patients,” the authors wrote.
Three of the SARS-CoV-2-positive patients developed fever while in hospital. Two were suspected to be endomyometritis – although one did not have any localised symptoms – and one fever case was linked to their COVID-19.
The authors pointed to the potential benefits of a universal testing approach for COVID-19, saying it could help determine hospital isolation and PPE practices, and inform neonatal care.
- Hypertension, diabetes and ischaemic heart disease are common comorbidities among patients who die from COVID-19, according to a research letter published in JAMA Network Open.
Of 168 patients who died from COVID-19 in 21 hospitals across Wuhan, China, three-quarters were men, all but seven were aged over 50 years, and the median age was 70 years.
Three-quarters of the patients had at least one comorbidity; half had hypertension, one-quarter had diabetes and 18.5% had ischaemic heart disease.
All the patients had been receiving oxygen therapy before they died, but only one in five were intubated and only two patients received extracorporeal membrane oxygenation treatment.
The authors said this suggested intubation was delayed for many patients, and cited a 2015 study showing that delayed intubation after failure of high-flow nasal oxygen or non-invasive ventilation was associated with increased mortality.
They wrote that the delay may have happened because some patients may not have shown symptoms of hypoxia, such as shortness of breath, but also that the lack of ventilators could also have prevented many of them being intubated.
10.05am, 14 April
- Here’s a bubble map of confirmed COVID-19 infections around NSW. [covid-19-graph]CurrentNumberofCOVID-19CasesbyNSWPostcode/BubbleMap[/covid-19-graph]
- The International Federation of Gynecology and Obstetrics has put out interim guidance on managing COVID-19 during pregnancy, which includes advice on monitoring, delivery and breastfeeding.
The paper, published in the International Journal of Obstetrics & Gynecology last week, suggests that while pregnant women are known to be more susceptible to severe illness after respiratory infection, there is so far no evidence that they are either more susceptible to COVID-19 or to COVID-19-related pneumonia.
Data collected from pregnant women with COVID-19 shows the most common symptoms of COVID-19 in pregnant women are fever and cough, two-thirds of women have lymphopaenia and elevated inflammatory markers, and the majority have multiple patches of ground-glass opacity on chest CT.
Both fever and viral pneumonia in early pregnancy have previously been linked to congenital structural abnormalities, preterm birth, foetal growth restriction, and perinatal mortality. But there’s no data so far on pregnancy outcomes after COVID-19 infections.
The paper’s authors advised that pregnant women with suspected, probable or confirmed COVID-19 should have a chest CT scan, and antenatal inspections and delivery should happen in a negative pressure isolation room.
They also recommended monitoring women’s oxygen saturation levels closely for signs of maternal hypoxia, and regular blood count, renal and liver function testing, and coagulation testing.
While there is so far no evidence of COVID-19 transmission from mother to baby, the authors said there wasn’t yet enough evidence to draw conclusions about the safety of breastfeeding. They advised that if the woman was well enough to breastfeed, she could do so.
- Some of Australia’s biggest pathology companies are pressuring GPs for rent reductions for co-located pathology labs, according to an article by The Medical Republic and the Guardian.
TMR has learned that Laverty Pathology and Western Diagnostics Pathology, both owned by pathology giant Healius, have been writing to clinics across the country asking for a 50% reduction in rent because of reduced demand for pathology testing.
The Australian General Practice Alliance has criticised the demands, saying they place additional financial pressures on already-struggling general practices.
“Most general practices rely on these pathology rents to remain viable,” AGPA Executive Officer Mr Richard Hart said in a statement. “In some cases this may make the difference between general practices remaining open or closing.”
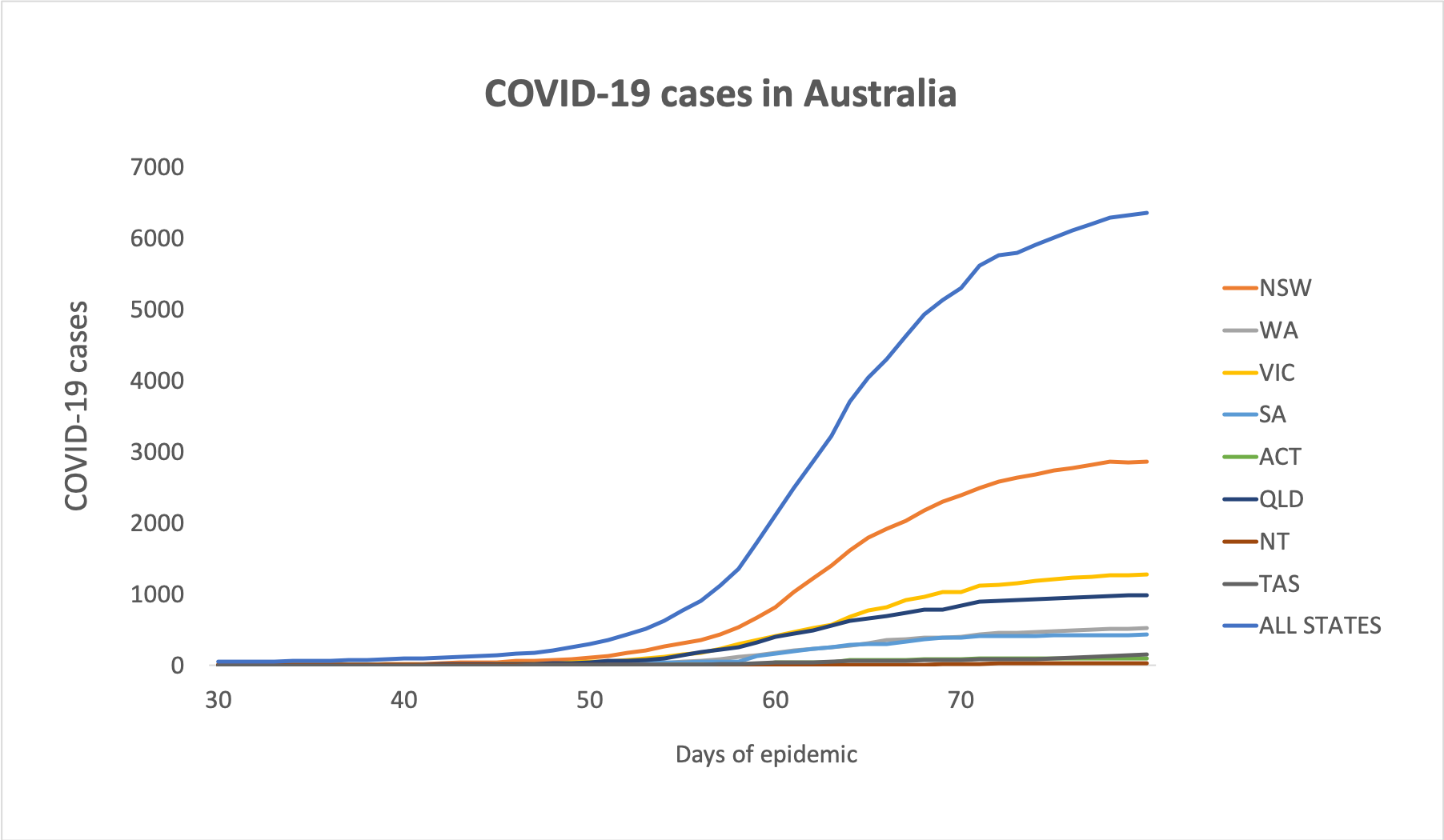
The move comes as Prime Minister Scott Morrison announced last week that that landlords would have to reduce rent for commercial businesses proportional to their loss in revenue. - Here are the latest statistics on confirmed COVID-19 infections in Australia, to 3pm yesterday:
National – 6,359 (up 46 since 3pm yesterday) and 61 deaths
ACT – 103
NSW – 2863
NT – 27
QLD – 987
SA – 431
TAS – 144
VIC – 1281
WA – 523
And here are some charts. The first is infections over time:
… by age group over time… [covid-19-graph]cumulative_covid19_cases_by_agegroup_over_time/caseloadovertimebyagegroup[/covid-19-graph]… and total NSW cases by age group. [covid-19-graph]TotalNSWCOVID-19casesbyAgeGroup/currentcaseloadbyagegroup[/covid-19-graph]
Disclaimer: The content on the Medical Republic COVID-19 blog is independently created by Medical Republic without input from Boehringer Ingelheim Pty Ltd. The views, information, or opinions expressed on the Medical Republic COVID-19 blog are Medical Republic’s own and do not necessarily represent those of Boehringer Ingelheim Pty Ltd. Boehringer Ingelheim Pty Ltd is not responsible for and does not verify the accuracy of any content on the Medical Republic COVID-19 blog.
